Medial epicondylitis (Golfer's elbow)
What is medial epicondylitis?
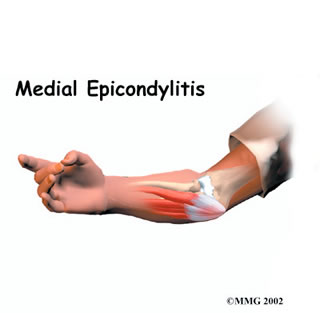
Medial epicondylitis is commonly known as golfer's elbow. This does not mean that only golfers have this condition. Many other repetitive activities can also lead to golfer's elbow: throwing, chopping wood with an ax, running a chain saw, and using many types of hand tools. It is pain that is caused by overuse of the tendons that attach to the part of the elbow called the medial epicondyle.
What parts of the elbow are affected?
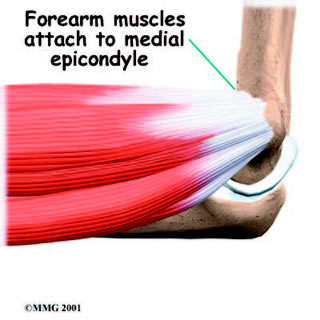
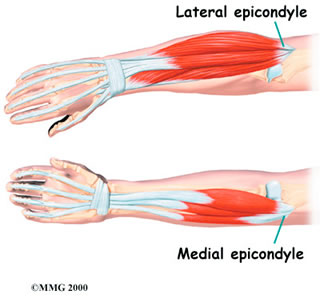
Golfer's elbow causes pain that starts on the inside bump of the elbow, the medial epicondyle. Wrist flexors are the muscles of the forearm that pull the hand forward. They attach to one main tendon on the medial epicondyle. This tendon is called the common flexor tendon. Tendons connect muscle to bone and when muscles work, they pull on the tendon. The other end of the tendon pulls on the bone, causing the bone to move. The wrist flexor muscles contract when you flex your wrist, twist your forearm down, or grip with your hand.
What causes medial epicondylitis?
 Overuse of the muscles and tendons of the forearm and elbow are the most common reason people develop golfer's elbow. Repeating some types of activities over and over again can put too much strain on the elbow tendons. These activities are not necessarily high-level sports competition. Shoveling, gardening, and hammering nails can all cause the pain of golfer's elbow. Swimmers who try to pick up speed by powering their arm through the water can also strain the flexor tendon at the elbow.
Overuse of the muscles and tendons of the forearm and elbow are the most common reason people develop golfer's elbow. Repeating some types of activities over and over again can put too much strain on the elbow tendons. These activities are not necessarily high-level sports competition. Shoveling, gardening, and hammering nails can all cause the pain of golfer's elbow. Swimmers who try to pick up speed by powering their arm through the water can also strain the flexor tendon at the elbow.
Constant strain and overuse keep re-injuring the tendon. After a while, the tendons stop trying to heal. The scar tissue that forms never has a chance to fully heal, leaving the injured areas weakened and painful.
What are the symptoms of medial epicondylitis?
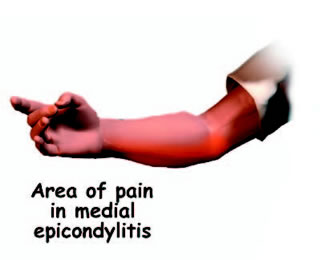 The main symptom of golfer's elbow is tenderness and pain at the medial epicondyle of the elbow. Pain usually starts at the medial epicondyle and may spread down the forearm. Bending your wrist, twisting your forearm down, or grasping objects can make the pain worse. You may feel less strength when grasping items or squeezing your hand into a fist.
The main symptom of golfer's elbow is tenderness and pain at the medial epicondyle of the elbow. Pain usually starts at the medial epicondyle and may spread down the forearm. Bending your wrist, twisting your forearm down, or grasping objects can make the pain worse. You may feel less strength when grasping items or squeezing your hand into a fist.
How is it diagnosed?
Your doctor will first take a detailed medical history. You will need to answer questions about your pain, how your pain affects you, your regular activities, and past injuries to your elbow. The physical exam is often most helpful in diagnosing golfer's elbow. Your doctor may position your wrist and arm so you feel a stretch on the forearm muscles and tendons. This is usually painful with golfer's elbow. Other tests for wrist and forearm strength are used to help your doctor diagnose golfer's elbow. You may need to get X-rays of your elbow. The X-rays mostly help your doctor rule out other problems with the elbow joint. Your doctor may suggest tests to rule out problems with the ulnar nerve. When the diagnosis is not clear, the doctor may order other special tests, such as a magnetic resonance imaging (MRI) scan or ultrasound.
What is the treatment?
Nonsurgical Treatment:
The goal of treatment is to help the tendon to heal. If the problem is caused by inflammation, antiinflammatory medications such as ibuprofen may give you some relief. If inflammation doesn't go away, your doctor may inject the elbow with cortisone. Cortisone is a powerful anti-inflammatory medication. Doctors commonly have their patients with golfer's elbow work with a physiotherapist. You may use an elbow strap that wraps around the upper forearm in a way that relieves the pressure on the tendon attachment. When symptoms are from a particular sport or work activity, your therapist will observe your style and motion with the activity. Your therapist may suggest ways to protect the elbow during your activities.
Surgical treatment:
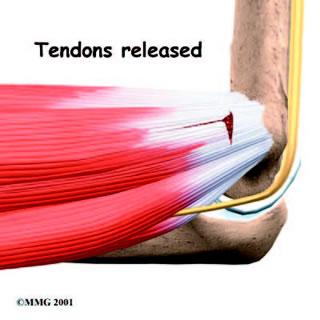
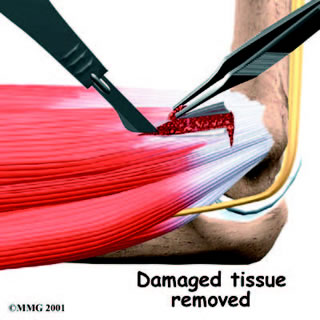
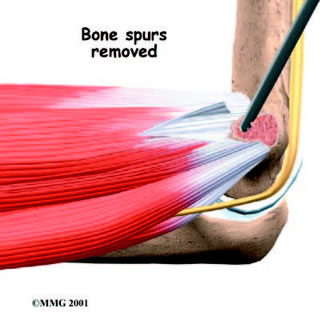
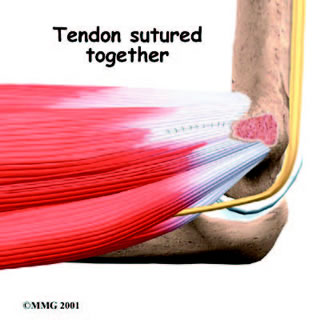
Sometimes nonsurgical treatment fails to stop the pain or help patients regain use of the elbow. In these cases, surgery may be necessary. A commonly used surgery for golfer's elbow is called a medial epicondyle release. This surgery takes tension off the flexor tendon. The surgeon begins by making an incision along the arm over the medial epicondyle. Soft tissues are gently moved aside so the surgeon can see the point where the flexor tendon attaches to the medial epicondyle. The flexor tendon is then cut where it connects to the medial epicondyle. The surgeon splits the tendon and takes out any extra scar tissue. Any bone spurs found on the medial epicondyle are removed.